Acupuncture and Carpal Tunnel Syndrome – CTS
Carpal tunnel syndrome is probably the most common nerve entrapment syndrome in the body and certainly the best known one. Nerve entrapment syndrome is called the condition in which a nerve trunk is compressed in a specific anatomical area by a specific anatomical structure. In the case of the carpal tunnel, this anatomical area is the curved configuration of the carpal bones, which create a groove. This groove is occupied by 9 tendons and the median nerve on their way to the hand.
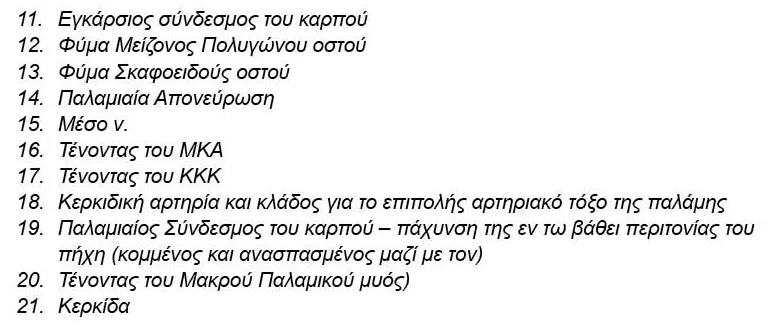
This groove is converted into a tube by the transverse carpal ligament, which acts as a roof and turns the groove into a closed rigid compartment. If for any reason the space of this compartment is diminished, the first anatomical structure to complain about the narrowness of the space is the median nerve, and symptoms include pain, numbness, a tingling sensation in the distribution area of the median nerve and characteristic nocturnal awakening.
The arsenal of Western medicine includes painkillers and anti-inflammatory drugs, immobilization with a splint either custom-made or off-the-shelf, nerve block, usually with a combination of local anesthetic and slow-acting cortisone, and, as a last resort, surgical treatment. Drugs are the usual first step and what a pharmacist would recommend. Following the exact same rationale, a physical therapist would recommend physical therapies. However, both rationales suffer, since the condition derives from a purely mechanical constraint.
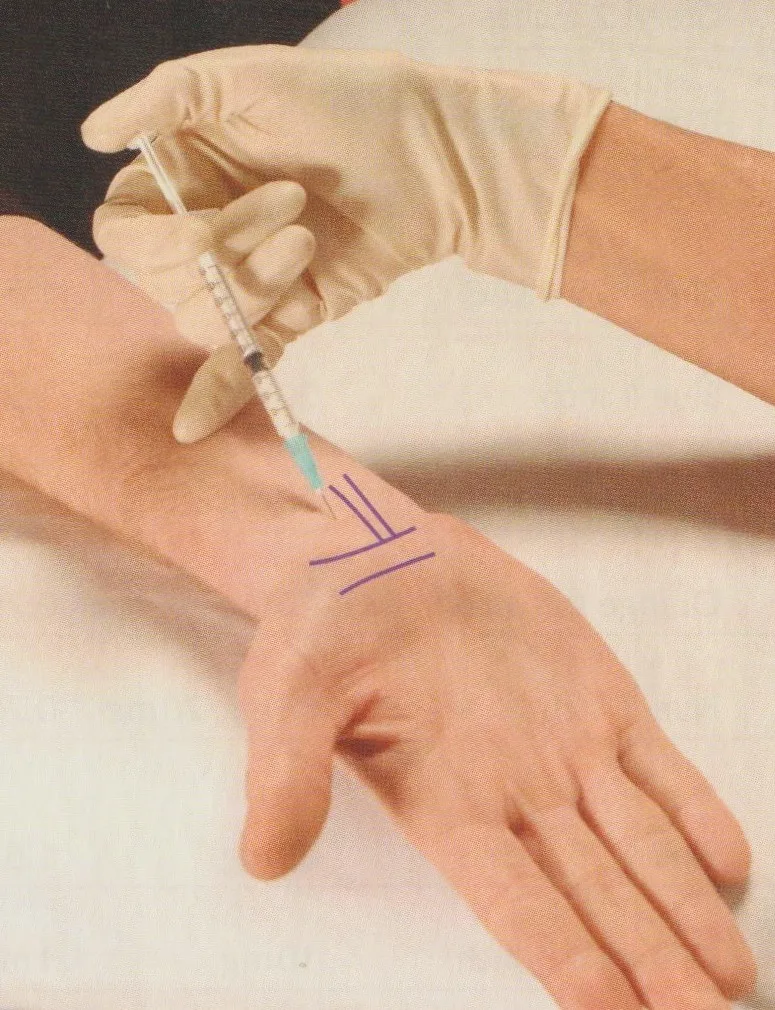
Immobilization and rest make sense as a temporary means of relief, but this is precisely the downside of the method, with relapses being the norm. Upon return to daily activities, the symptoms return. The local injection of medicinal substances, aka wet needling, may also be considered, with the choice of an anesthetic for blocking the pain receptors, and a slow-acting cortisone preparation for reducing local inflammation.
In contrast, the rationale for systemic administration of cortisone suffers structurally, as in addition to its strong anti-inflammatory effect, cortisone causes significant fluid retention and consequent tissue swelling. After all, this is thought to be the dominant pathogenetic mechanism for the increased incidence of CTS during pregnancy, where patience is probably the best course of action. Once the flood of hormones subsides, the symptoms of CTS typically subside.
When conservative treatment fails, then the Orthopedic, General or Plastic surgeon will recommend the final solution, releasing the transverse ligament of the wrist and relieving the median nerve from the constant pressure. The reasoning is exactly what was mentioned above for other professional groups. Thus, a surgeon “must” recommend surgical treatment and usually does so gladly. The problem is that his joy is not shared by most patients, with the occurrence of “doctor shopping” showing alarming proportions, as many patients refuse to undergo surgery and insist on looking for some less aggressive treatment.
Acupuncture may offer an alternative solution, especially in mild and moderate cases, as long as it is mentioned as one of the available options. The method is minimally invasive, requires a few sessions depending on the severity and especially the chronicity of the condition, but its main issue is compensation by public or private insurance. Thus, patients who already pay the mandatory state as well as the optional private insurance resent the possibility of further financial burden and often directly choose the more drastic solution, which is covered by insurance, over the milder solution, which is not covered by insurance and requires out of pocket money.
However, Orthopedic Surgeons who use acupuncture as part of their armamentarium automatically gain a significant advantage, as they are able to present their patient with two solutions instead of the usual one and only. Current Medical Ethics consider the physician as the patient’s consultant for his specific medical condition. As a consultant, any physician must provide full information to his patient and let him decide. The decision, after full and honest information, now belongs to the patient, not the treating physician. The responsibility of the attending physician is exhausted in full and honest information, presenting all the advantages and disadvantages of ALL methods.
After all, a key component of this scenario is that the physician is remunerated by the patient (or his insurance) precisely for this reason, the complete and honest citation of ALL options. Unfortunately, none of the parties involved, patients, doctors and insurance companies, really want this scenario, in which decision-making is the exclusive right of the patient and no one else. If the patient finally chooses the acupuncture solution, the treatment can be purely Eastern, with a complete Oriental history taking (the famous 20 questions), a complete clinical examination, especially of the pulse and tongue, classification of the patient according to the Five Elements or Phases and subsequent personalized treatment of the patient as a whole. This scenario is considered rather rare among physician acupuncturists, but is prevalent among non-physician acupuncturists.
Alternatively, if the patient does not wish to undergo surgery, the acupuncturist, ideally the Orthopedic Surgeon – Medical Acupuncturist, will proceed with acupuncture treatment, stressing that the possibility of operative treatment is still there, should the method fail. However, since acupuncture is a mild intervention, the possibility of future recurrence cannot be ruled out and should be disclosed from the very beginning. Furthermore, the exact number of sessions required cannot be accurately calculated in advance. A solution to this may be the initial remuneration of the overall treatment, regardless of the number of sessions eventually required.
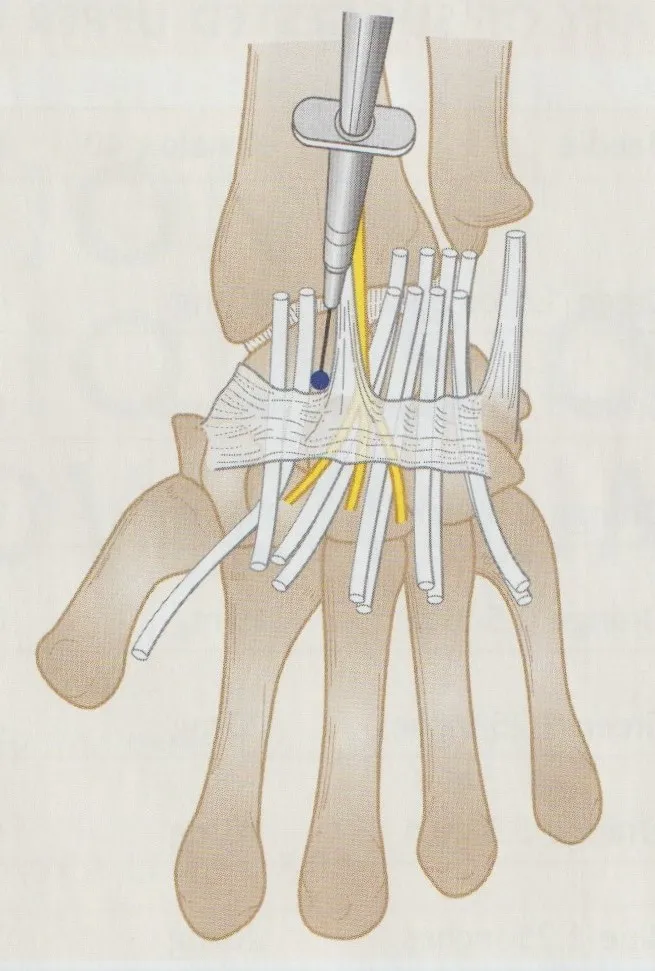
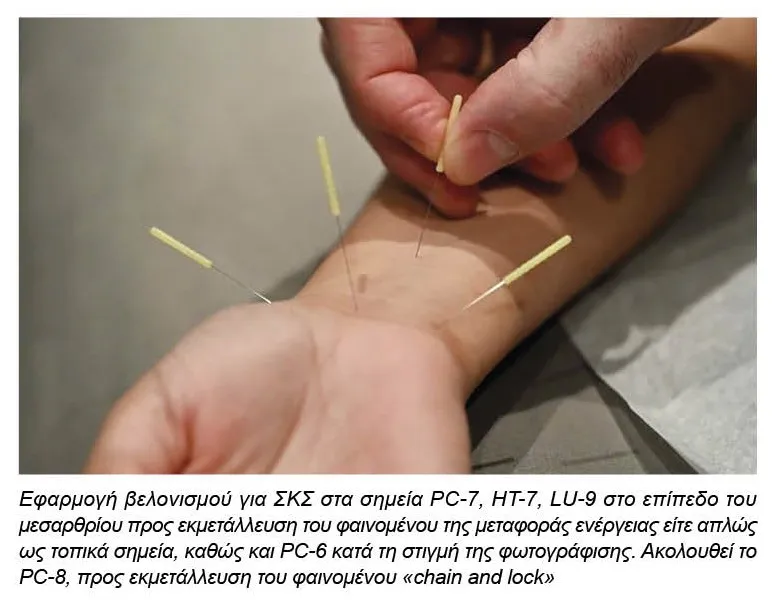
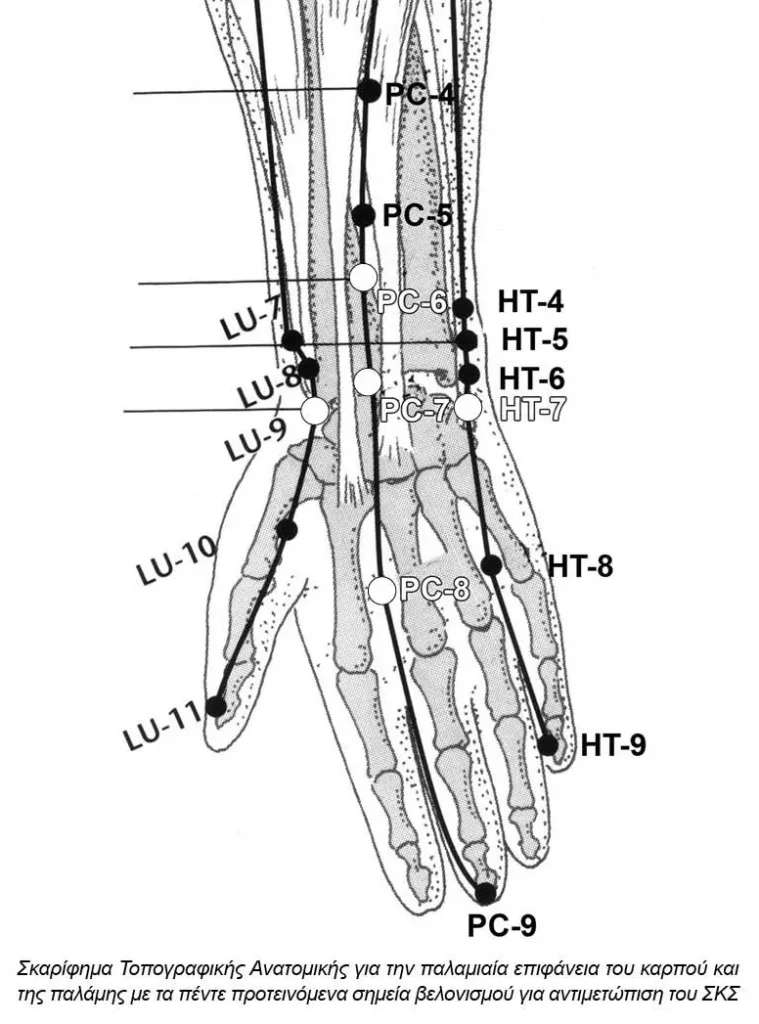
Several differing forms of acupuncture are reviewed in the literature, with the final conclusion being ambiguous. Most papers deal with traditional body acupuncture, some of them electro-acupuncture and rather recently laser acupuncture. Several researchers follow a personalized approach, while others follow a standardized approach, which the latter allowing for easier interpretation of the results. Acupuncture sessions are usually done twice or thrice a week and strong needles are required. Point selection must include the Pericardium meridian, with the acupuncture point PC-7, in 100% of cases, followed by PC-6 and then PC-8, in a micro-application of the “chain and lock” method.
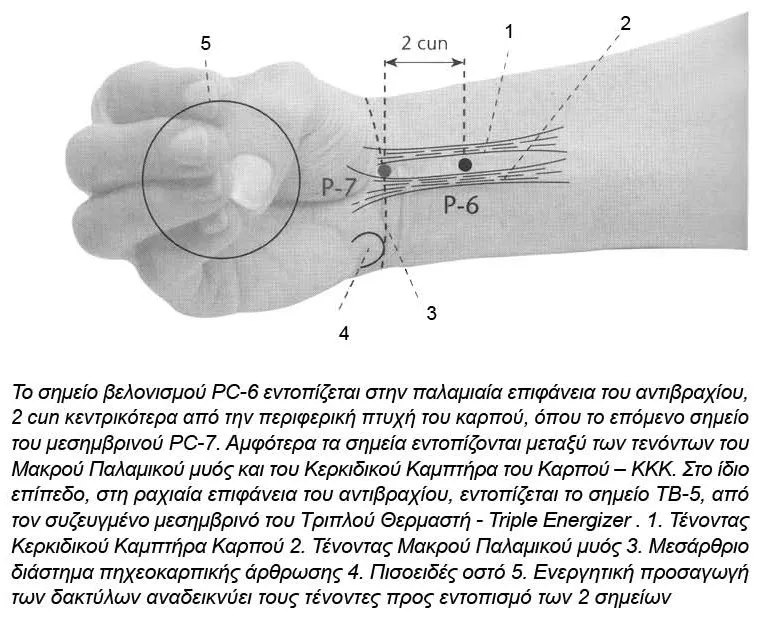
Other selected acupoints include LI-4 and LI-11, as well as points from adjacent meridians, like the LU and HT meridians, located on the wrist crease, namely LU-9 and HT-7. This way, only 5 needles on each side are enough, with the treatment involving either the affected limb alone, the opposite limb or both.
Caution is advised regarding strong manipulation in a closed compartment, which is the initial cause of the syndrome. Bleeding into this compartment can worsen, or in rare cases create de novo, pressure symptoms. Closed compartments, rigorous manipulation in the vicinity of vessels, acupuncture therapy in patients receiving anticoagulants warrant increased attention. CTS, usually considered a benign condition and easy to treat, may present with severe complications and adverse effects. Based on common sense, acupuncture should be reserved for mild to moderate cases of CTS.
Recommendation of acupuncture in severe cases, especially when atrophy of the thenar muscles is already present, ceases to be an attempt to combine Western and Eastern medicine and flirts with malpractice. However, in case of established atrophy in chronic cases, even the operative release of the transverse ligament does not guarantee a full recovery.